
INTRODUCTION
The novel coronavirus of 2019 (COVID-19) pandemic continues to spread in the United States and around the world. The United States, as of April 11, 2021, recorded 31.1 million COVID-19 cases and 561 231 deaths.1 Cases and deaths in the United States continue to account for the largest share of global cases (23%) and global deaths (19%).2 Containing the COVID-19 pandemic in the United States was challenging due to virus contagion characteristics, its pathophysiology, and socio-political factors.3 In response to the pandemic, many states initially adopted safety measures such as mask mandates, social distancing and safety measures for operations of certain businesses.4,5 After implementing these restrictive measures including lockdowns, many states rolled back such policies in 2020.6 Despite these rollbacks, personal safety measures (mask mandates and social distancing) were continued into the year 2021. However, as of the writing of this study, 14 states in the United States have lifted mask mandates.7
Safety measures such as the closure of business establishments, stay-at-home orders, and social distancing mandates severely impacted the economy.8 In response to the pandemic, lawmakers passed three stimulus packages and the Coronavirus Aid, Relief, and Economic Security Act (CARES) Act, with additional relief legislation expected.9,10 As of April 11, 2021, Moderna, Pfizer, and Johnson & Johnson vaccines have received emergency use authorization by the US Food and Drug Administration and are being rolled out in phases. Other biopharmaceutical companies are conducting clinical trials for 60 COVID-19 vaccine candidates.11 The current vaccine rollout will continue to gain momentum while other COVID-19 vaccines may receive market approval in the near future. Despite this progress, experts recommend that the public follow COVID-19 safety measures due to slow initial rollout, uncertainties surrounding COVID-19 vaccines (virus mutations, duration of immunity, real world effectiveness, vaccine uptake, etc.) and vaccine hesitancy.12,13 In summary, the US government and the scientific community has undertaken various measures to address the needs of the population during the COVID-19 pandemic. However, the assessment of the impact of ecological contextual factors such as health behaviors, clinical care and burden, socio-economic, and physical environment-related characteristics on the course of the COVID-19 pandemic is necessary. The contextual understanding from such a study is required to gauge whether lock-down measures worked and to what extent. Moreover, the study also aids in identifying high-risk areas for targeting vaccine distribution. Therefore, having a thorough knowledge of these ecological contextual factors is critical to address the public health and economic challenges and prioritize resources.
Studies so far have generated predictive models for growth in COVID-19 incidence and mortality and estimated the impacts of some community-level factors on COVID-19 incidence and mortality. Millett et al. and Khanijahani et al. focused on assessing the ecological determinants of susceptibility to COVID-19 outcomes among predominantly African American counties, while Fielding-Miller et al. and Peters et al. performed a similar assessment along the rural-urban continuum.14–17 Few studies have assessed the spatial determinants of COVID-19 transmission.3,18,19 Recently, Sun et al. assessed the relationship between various county-level determinants and COVID-19 incidence while Andersen et al. also identified high prevalence clusters.3,18 These studies evaluated the incidence and prevalence during the initial phase of the pandemic and limited the analysis to a few county-level and policy-related factors.
Incidence and mortality were critical outcomes in shaping the initial pandemic response to reduce the contagion. However, to reduce fatalities in the current stage of the pandemic, an increasing focus is placed on mitigation strategies such as increasing vaccination rates and continuing safety precautions such as social distancing and mask use. Therefore, COVID-19 case-fatality rate (CFR) is a useful outcomes measure in the current stage of the pandemic. CFR, being less susceptible to testing and reporting biases, also reflects the disease severity. In a study led by author Cao, country-level demographic and socioeconomic characteristics on COVID-19 CFR were presented.20 However, to our knowledge, in the United States, no study has estimated the effect of county-level ecological factors, including policy-related factors, on COVID-19 CFR.
The objective of the current study was to assess the impact of county-level ecological factors, using spatial econometric analysis, on the COVID-19 CFR over one year of the pandemic.
METHODS
Data source and study design
The current study used county-level COVID-19 confirmed cases and deaths data from the New York Times repository extracted as of February 27, 2021, and included data up until that date.18 The study used county-level characteristics from 2020 County Health Rankings data and 2018-2019 Area Health Resource File data. State-level stringency index, percent positive for COVID-19, and social distancing score were obtained from Oxford COVID-19 government response tracker, the COVID Tracking Project, and Unacast, respectively.4,21–24 Alaska and Hawaii counties were excluded from the analysis. The US counties ESRI Shapefile was obtained from the US Census Bureau.25 The study employed a cross-sectional ecological study design to assess the association between county-level characteristics on the cumulative COVID-19 CFR.
Outcomes
The county-level US COVID-19 cumulative confirmed cases and deaths data from the New York Times repository was extracted as of February 27, 2021, data up until that date was included.18 The COVID-19 cumulative CFR was operationally defined as a ratio of the cumulative COVID-19 deaths by cumulative COVID-19 cases.20 The current analysis used CFR as the outcome of interest because it reflects the disease severity, treatment effectiveness, and responsiveness of the health-care system.20 Additionally, since the measure is a ratio, compared to incidence rate or mortality rate, the CFR is less sensitive to differences in testing rates across regions.
Covariates
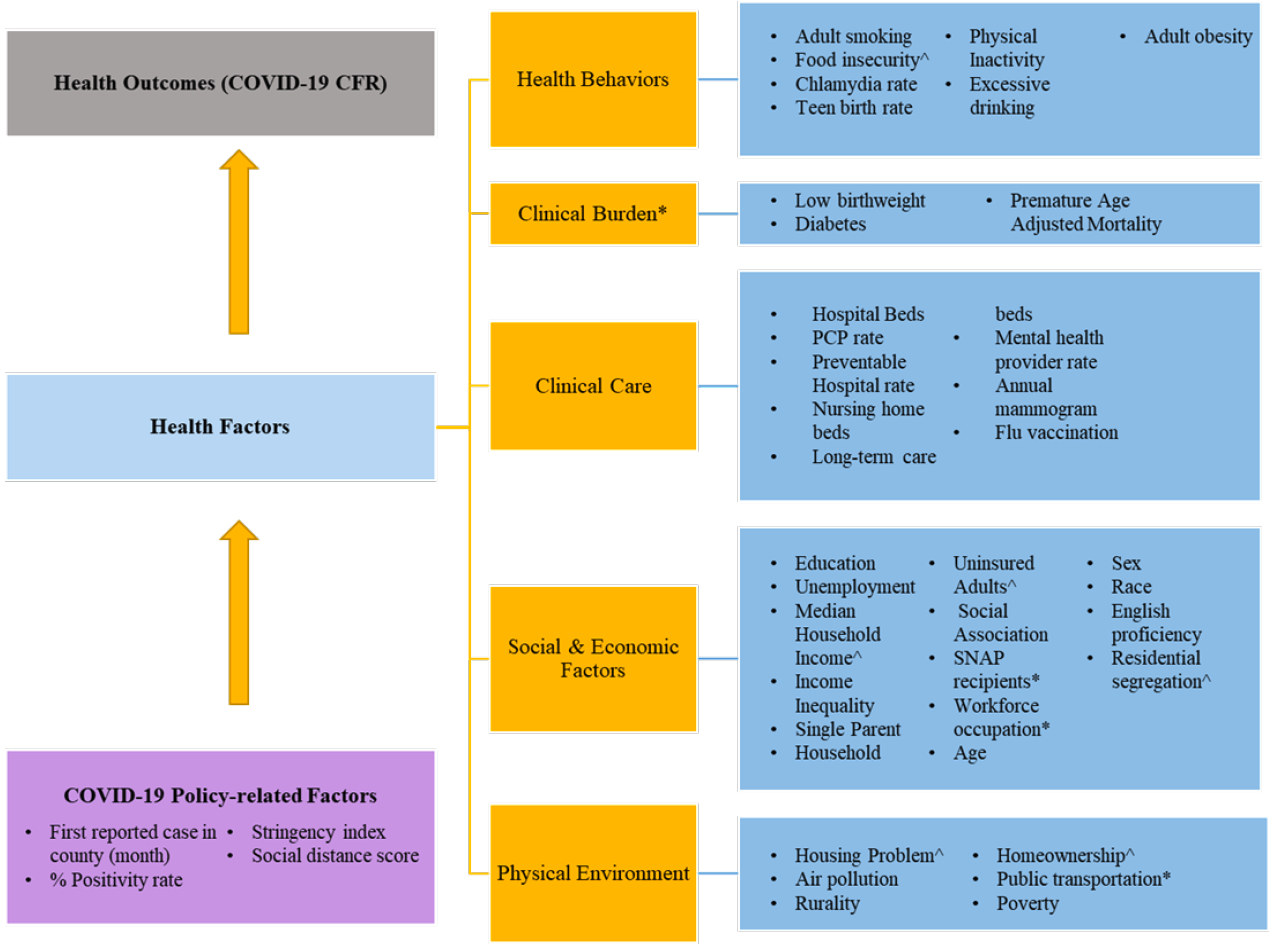
The covariates selected within the model to predict the county-level CFR were adapted from the County Health Ranking Framework (CHRF).26 The framework categorizes health factors into four sub-categories, namely health behaviors, clinical care, socioeconomic factors, and physical environment (Figure 1). Each of the sub-categories is further divided into individual factors. The CHRF model was used in the current analysis because it provides a well-established theoretical framework for studying ecological determinants of health outcomes. The current analysis augmented the CHRF by including additional covariates based on additional demographic measures from county health ranking, and prior ecological studies on COVID-19. Firstly, an additional sub-category of “clinical burden” was added, which included measures such as low- birth weight, percent diabetes prevalence, and premature age-adjusted mortality. Secondly, nursing home beds, long-term care beds, and total hospital beds were added to the clinical care sub-category.3 Thirdly, population characteristics such as rurality, poverty, age distribution, population, population density, supplemental nutritional assistance program (SNAP) eligibility, and percentage of workforce in various occupational categories were added to the social and economic factors sub-category.3,15,18,27,28 Additionally, physical environmental factors such as percentage of workers using public transport, were added to the respective sub-category.28 Finally, COVID-19 related factors were added to the model, which included month of first infection in the county, positivity rate for COVID-19 at the state-level, social distancing score, and stringency index.3,4,20–23,29 The final list of potential county-level covariates and corresponding rationale are described in Table 1. Although the CHRF model assigns weight to each of the components, they were not utilized in the current analysis as no composite rank score was calculated.

Statistical Analyses
Descriptive univariate statistics of the weighted county-level characteristics were generated. Firstly, all covariates in Table 1, selected as potential covariates, underwent a two-step covariate selection process. In the first step, multicollinearity was assessed and factors with variance inflation factor >7 were excluded.31 In the second step, Pearson correlation between remaining factors was tested (Supplemental Table 1) and factors with correlation greater than 0.7 were excluded.20 All remaining factors were used in regression analysis. Secondly, the presence of spatial correlation was confirmed by performing Moran’s I test for spatial correlation. Two island counties were excluded because spatial regression analysis necessitates that the data contains no island counties. Based on prior research, the LeSage and Pace method was used to determine the best fit spatial regression model.30 A first-order queen spatial weight matrix was employed for all spatial models. The queen matrix defines neighbor relationships if the counties either share a border or a vertex. All analysis was performed in RStudio (R) v 4.0.3 (Boston, Massachusetts) and QGIS v 3.16.0 (Berne, Switzerland).
RESULTS
The final analysis included data from 3101 counties from the mainland United States. Between January 20, 2020 to February 27, 2021, the population-weighted COVID-19 CFR for the mainland United States was 1.82%. Table 2 demonstrates the descriptive statistics of the COVID-19 CFR and county-level determinants, namely, COVID-19 policy-related factors, health behaviors, clinical burden, clinical care, socio-economic, and physical environment factors. Some 2097 counties reported their first case in March 2020. The percent positivity for COVID-19 was 9%. The mean social distance score and stringency index at the county-level was 1.75 and 49.14, respectively. The proportion of adult smokers, those with physical inactivity, obesity, and Medicare enrollees who were administered influenza vaccines were 15%, 23%, 29%, and 46%, respectively. At the county- level, the average ratio of population to primary care physicians was 74 and the average preventable hospitalization rate was 4545 per 10 000 Medicare enrollees. Premature age-adjusted mortality was 342 per 100 000. Among socio-economic factors, the proportion of the workforce in education/health-care/social assistance field, construction, and manufacturing comprised 23%, 7%, and 10% of the population, respectively. Additionally, unemployment was 4%, 12% of adults were uninsured, the mean income inequality ratio was 5 and adults with some college education made up 65% of the population. About 13% were African Americans, 18% Hispanics, 1% Native Americans, 51% females, 33% of the children lived in single-parent households, and 4% of the population was not proficient in English. The percentage of the population older than 65 years and less than 18 years were 16% and 22%, respectively. On average, 19% of counties were rural, the homeownership rate was 64%, 18% used public transportation and 18% of households had severe housing problems. Lastly, population density/100 sq. miles was found to be 2067.
Figure 2 presents the spatial distribution (quintiles) of COVID-19 CFR. In the West, Washington’s Spokane area and Nevada’s Las Vegas area had high COVID-19 CFR. High COVID-19 CFR clusters were found in border counties of Arizona’s Phoenix area and in New Mexico. In Montana, all major cities such as Helena, Butte, and Billings and along the border of Wyoming (specifically near Yellow Stone National Park) had high COVID-19 CFR. In the Midwestern region, barring the high COVID-19 CFR clusters in Michigan’s Upper Peninsula area, there were many scattered counties with high CFR. The Deep South states of Mississippi, Louisiana, Tennessee, central Alabama, and Arkansas had clusters of high COVID-19 CFR. The Texas panhandle region, the Corpus Christie, Texas, area and the area along the US-Mexico border had clusters of high COVID-19 CFR. In the Northeastern region, high COVID-19 CFR clusters were found between the large parts of Pennsylvania and New Jersey, and in the Boston, Massachusetts, area. Additionally, in Maine, clusters of high COVID-19 CFR were found around Acadia National Park and the northeastern parts of the state.

The first step in the factor selection process identified and excluded percent adult smokers, percent fair/poor health, log population density, log population, percent under poverty, median income, percent eligible for SNAP benefits due to multicollinearity, which is shown in Table 2. Similarly, percent smokers, teen birth rate, percent SNAP eligible, log population, log population density, percent speaking language other than English were excluded based on high correlation with other factors (Supplemental Table 1). The presence of spatial autocorrelation was confirmed based on a significant Moran’s I test statistic (Moran’s I=0.256, P-value<0.001). The LeSage and Pace method identified that Spatial Durbin Model (SDM) was a better fit to the data compared with other spatial regression models. The significant Rho parameter of the SDM model indicates that (Rho=0.447, P-value<0.001), a 1% increase in a neighboring county’s CFR, also results in 0.447% increase in CFR rate in the particular county.
The multivariable SDM results are presented in Table 3. The factors significantly associated with CFR included percent positive for COVID-19 (β=0.059), stringency index (β=0.015), log nursing home beds (β=-0.005), log long-term care beds (β=0.008), percent workforce in construction (β=-0.019), log premature age-adjusted mortality (β=0.711), income inequality ratio (β=0.076), percent population 65 years and older (β=0.055), and percent severe housing problem (β=-0.023). Additionally, the spatial lag term for factors such as percent positive for COVID-19 (lag β=-0.048), stringency index (lag β=- 0.017), social distancing score (lag β=-0.136), adult obesity (lag β=-0.026), log long-term care bed (lag β=0.025), log mental health provider rate (lag β=-0.080), percent workforce in education/health-care/social assistance (lag β=0.018), log social association rate (lag β=0.038), percent female (lag β=-0.057), and percent rurality (lag β=0.005) were also associated with COVID-19 CFR.
As the β from SDM are not directly interpretable, the estimates from the SDM were decomposed into direct and indirect effects using the Impacts command from spdep package as shown in Table 3.30,32 Several factors had significant direct impact on the county’s COVID-19 CFR. Firstly, two of the COVID-19 related factors, namely, percent positive for COVID-19 (direct impact: 0.057% point), and stringency index (direct impact: 0.014% point) were positively associated were higher COVID-19 CFR in that county. Secondly, among health behavior related factors, percent adult obesity (direct impact: -0.013% point) was negatively associated with COVID-19 CFR. Thirdly, among the clinical burden and clinical care related factors, percent diabetics (direct impact: 0.011% point), log premature age-adjusted mortality (direct impact: 0.702% point), and log long-term care beds (direct impact: 0.010% point) were positively associated with COVID-19 CFR, while log nursing home beds (direct impact: -0.005% point) was negatively associated with COVID-19 CFR. Several socio-economic factors, importantly, income inequality (direct impact: 0.078% point), log social association rate (direct impact: 0.014% point), and percentage African Americans (direct impact: 0.007% point) were positively associated with COVID-19 CFR, while percentage workforce in construction (direct impact: -0.024% point) and percentage adults with some college education (direct impact: -0.004% point) were negatively associated with COVID-19 CFR.
The decomposition estimates also demonstrated strong indirect effects of spatial lag terms indicating externality associated with ecological factors from surrounding counties on COVID-19 CFR. The directionality of the direct and indirect associations was similar for the majority of the factors. However, some of the factors demonstrated divergent direct and indirect effects on COVID-19 CFR. For illustration, among COVID-19 policy-related factors, both percent positive for COVID-19 (direct: 0.057% point; indirect impact: -0.035% point) and stringency index (direct impact: 0.014% point; indirect impact: -0.017% point) of neighboring counties were negatively associated with COVID-19 CFR in a given county. Interestingly, the magnitude of the indirect associations were larger than the direct associations for the majority of the factors, except for percent 65 years old and over (direct: 0.055% point; indirect: 0.024% point), and percent severe housing problem (direct: -0.024% point; indirect: -0.009% point).
It is noteworthy that for some of the factors, while either the direct or indirect impacts were insignificant, the total impact was found to be significant: for example, food insecurity (total impact: 0.160), log of mental health provider rate (total impact: -0.146% point), percent of workforce in education/health-care/social assistance field (total impact: 0.045% point), percent uninsured adults (total impact: 0.028% point), percent 65 years old and over (total impact: 0.079% point), residential segregation non-White/White (total impact: 0.015% point), and percent rural (total impact: 0.007% point). For percent excessive drinking factor, although the direct and indirect impacts were found to be insignificant, the overall total impact (0.043% point) was significant.
DISCUSSION
To the best of our knowledge, this is the first spatial analysis study that captured and assessed the COVID-19 CFR through the year 2020-2021 (January 20, 2020 to February 27, 2021) of the COVID-19 pandemic in the United States. The study found that both direct and indirect impacts of food insecurity, diabetes, long-term care beds, and social association rate on COVID-19 CFR was positive. However, only the direct impact of stringency index, premature age-adjusted rate, income inequality ratio, population aged 65 years or more, and African Americans on COVID-19 CFR was significant and positive. Conversely, both the direct and indirect impacts of proportion of adults with obesity, mental health provider rate, workforce in construction, and adults with some college education on COVID-19 CFR was negative. While factors such as nursing home beds and severe housing problem had a negative direct impact on COVID-19 CFR, stringency index and percent females were found to have a negative indirect impact on COVID-19 CFR.
Only one study by Cao et al has assessed the ecological determinants of COVID-19 CFR but that study used country-level data.20 Similar to our study, Cao et al reported that stringency index and diabetes prevalence were associated with higher CFR. Although no US-based studies have assessed an association between county-level ecological factors and COVID-19 CFR, some studies have reported on the ecological determinants on COVID-19 mortality. A few studies have reported high deaths in counties with greater proportions of racial minorities (Hispanics and African Americans) and found results similar to the present study.15,33 Stokes et al found that greater proportions of income inequality ratio and African American population was associated with high death rates, which is similar to the relationship this study found with CFR as an outcome.29
Aside from the similarities with already published literature on COVID-19, this study adds to the literature on ecological determinants of COVID-19 CFR. Firstly, this study demonstrated a positive association between percent positive for COVID-19 and COVID-19 CFR. Percent positive for COVID-19 captures both community level transmission rate and inadequacy of testing.34 Hence, increased community-level testing and timely local-level lockdown policies may be needed to improve CFR. Surprisingly, the indirect impact of percent positive for COVID-19 was negative, which warrants further research. Secondly, unlike Cao et al, this study found that a higher stringency index in neighboring counties was significantly associated with lower COVID-19 CFR in a given county. However, unlike the indirect association, the direct association between stringency index and COVID-19 CFR was positive due to endogeneity. For illustration, states such as New York and Washington were the early hotspots for COVID-19 cases and deaths.4 As a result, due to early lockdown policies that lasted for a long duration, these states had higher stringency index values.6 Thirdly, workforce composition in a given county and its surrounding counties were also associated with COVID-19 CFR. Finally, our study found very strong positive association between premature age-adjusted mortality and COVID-19 CFR in a given county. Numerous studies have assessed determinants of premature age-adjusted mortality. Based on the research, public health interventions aimed at reducing premature age-adjusted mortality would also play a vital role in reducing COVID-19 CFR. The study has important limitations. Given the study is cross-sectional and ecological in nature no causal inferences or inferences at the individual level can be made. Although our study included percent positive for COVID-19, there are considerable differences in the testing rates across regions. Relative to incidence and mortality rates, the CFR is less sensitive to testing rates. However, if differential bias in testing of incidence and mortality rates persists then CFR may be biased. Even though stringency index and social distancing scores are included in the study, these measurements were taken at a specific time point. Further, the list of variables is by no means comprehensive and does not include several other factors such as local safety policies (county or city level), and compliance with local and federal prevention guidelines.
CONCLUSION
The findings of this study are more insightful than the mere coronavirus count meters and data visualizations that depict the spread of the COVID-19 pandemic. The current spatial models incorporated a comprehensive list of factors to ensure that the results, when parsed, offer a multi-faceted explanatory power. For illustration, these models helped identify factors including COVID-19 policy-related factors (stringency index, social distancing score, and percent positive for COVID-19), health behaviors (example: excessive drinking), clinical burden (example: percent diabetic, premature age-adjusted mortality), clinical care (example: mental health provider rates), socio-economic factors (example: race/ethnicity, income inequality, segregation index, education, workforce composition), and physical environment (example: rurality) as some of the important determinants of the geographic disparities in COVID-19 CFR. This study highlights the plausible effect of one’s residential location, vicinity, local state policy and the connectivity to the neighboring counties on COVID-19 CFR. The United States is facing the next set of challenges in limiting fatalities and COVID-19 mutations, while undertaking mass immunization for COVID-19. At this crucial juncture, the current study findings provide guidance on identifying areas at greater risk of COVID-19 CFR.
ACKNOWLEDGEMENTS
We would like to thank the New York Times for providing us with the data, which was based on reports from state and local health agencies.
FUNDING
The study received no funding.
CONFLICTS OF INTEREST
The authors declare no competing interests.
CONSENT FOR PUBLICATION
All authors have consented for this manuscript to be published.
COMPETING INTERESTS
None.
AUTHORS’ CONTRIBUTIONS
NK and RW conceived and designed the study; NK and RW collected, cleaned, and curated the data; NK and RW conducted the statistical analysis. NK and RW discussed the results, interpreted the data, and modified the first manuscript. NK and RW supervised the data collection and interpreted the data. Both the authors have read and gave final approval for publication.